Surgeon: Aakriti Garg Shukla, MD | Narrator: Lindsay Machen, MD | Year: 2019
PREOPERATIVE DIAGNOSIS:
Glaucoma with failed filtering bleb, *** eyePOSTOPERATIVE DIAGNOSIS:
SamePROCEDURE PERFORMED:
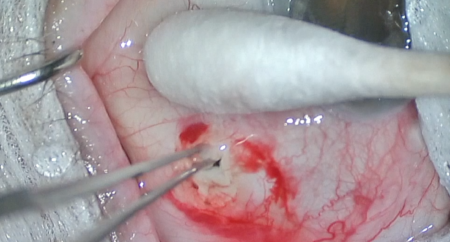
Bleb needling with mitomycin-C, *** eyeATTENDING SURGEON:
***ASSISTANT SURGEON:
***ANESTHESIA:
MAC, topical, and localCOMPLICATIONS:
NonePrior to the date of surgery, the risks, benefits, and alternatives of the planned procedure were discussed with the patient, and informed consent was obtained. The patient was identified in the preoperative area by the attending physician, and the operative eye was marked. The patient was taken to the operative suite and given IV sedation and topical ocular anesthesia. The operative eye was prepped and draped in the usual sterile ophthalmic fashion. A lid speculum was inserted.
A sub-Tenon’s block of equal parts lidocaine and bupivacaine was given in the inferotemporal quadrant. An 8-0 silk traction suture was placed in partial-thickness superior cornea, and the eye was rotated inferiorly to enhance exposure. A paracentesis was made into clear cornea. An anterior chamber maintainer was placed. A bent 25-gauge needle was advanced in the subconjunctival space adjacent to the scleral flap and used to break the episcleral adhesions and lift the flap, entering the anterior chamber. The bleb was noted to elevate well. Mitomycin-C (0.4 mg/mL) was injected in the subconjunctival space adjacent to the bleb.
The traction suture and anterior chamber maintainer were removed. The corneal incision was hydrated then inspected with a Weck-cel sponge and found to be watertight with good intraocular pressure by finger tension. The speculum and drapes were removed, and antibiotic-steroid drops were placed in the eye. A patch and shield were applied. The patient was then transported to the postoperative care unit in good condition.