Surgeon: David Xu, MD | Year: 2019
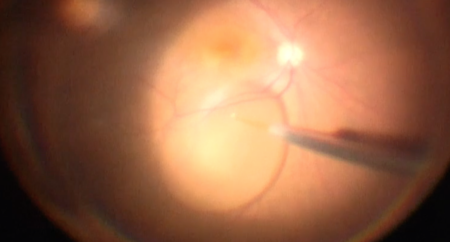
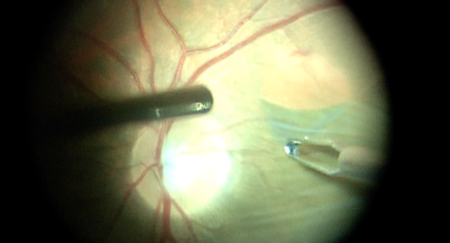
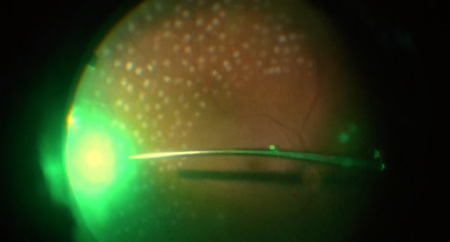
Dr. Xu implants a scleral buckle to treat a rhegmatogenous retinal detachment in a phakic patient.
PREOPERATIVE DIAGNOSIS:
Rhegmatogenous retinal detachment, *** eyePOSTOPERATIVE DIAGNOSIS:
SamePROCEDURE PERFORMED:
Scleral buckle, *** eyeATTENDING SURGEON:
***ASSISTANT SURGEON:
***IMPLANT:
Scleral buckle, serial number ***ANESTHESIA:
General and localCOMPLICATIONS:
NonePrior to the date of surgery, the risks, benefits, and alternatives of the planned procedure were discussed with the patient, and informed consent was obtained. The patient was identified in the preoperative area by the attending physician, and the operative eye was marked. The patient was taken to the operative suite and given IV sedation and topical ocular anesthesia. The operative eye was prepped and draped in the usual sterile ophthalmic fashion. A lid speculum was inserted.
A 360-degree conjunctival peritomy was performed using Westcott and Stevens scissors. A sub-Tenon’s block consisting of a 50:50 mixture of mepivacaine and bupivacaine was given. A Gass muscle hook was used to identify the insertions of all four rectus muscles, then separate 4-0 silk sutures were passed beneath each muscle to serve as traction sutures. The sclera was inspected in the exposed quadrants and found to be healthy without significant thinning. A #41 scleral buckle was passed under the rectus muscles and anchored using 5-0 nylon sutures. The ends of the buckle were secured in the superonasal quadrant with a #70 sleeve.
The conjunctiva was then repositioned over the globe and closed with interrupted 6-0 plain sutures. The speculum and drapes were removed, antibiotic-steroid drops were placed in the eye, and a patch and shield were placed over the eye. The patient was then transported to the recovery unit in stable condition.