Surgeon: David Xu, MD | Year: 2019
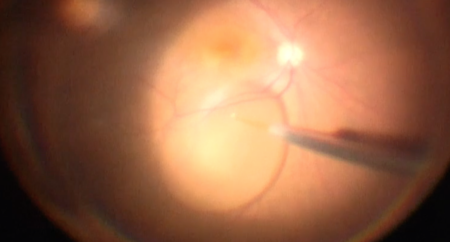
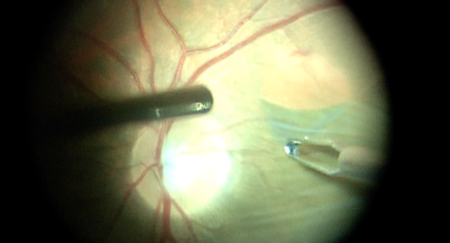
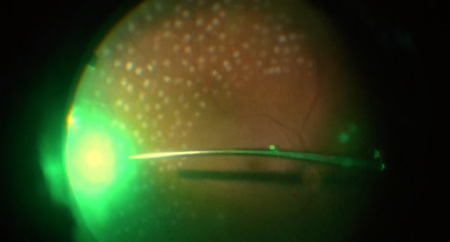
Dr. Xu performs a pars plana vitrectomy for vitreous floaters. First, a sub-Tenon’s block is given. Next, three vitrectomy ports are placed 4 mm from the limbus in this phakic patient. Next, a core vitrectomy is performed, followed by a thorough shave of the vitreous base. Scleral depression is performed, and retinal tufts are treated with endolaser. Finally, an air-fluid exchange is done, then the ports are removed.
PREOPERATIVE DIAGNOSIS:
Vitreous floaters, *** eyePOSTOPERATIVE DIAGNOSIS:
SamePROCEDURE PERFORMED:
Pars plana vitrectomy, *** eyeATTENDING SURGEON:
***ASSISTANT SURGEON:
***ANESTHESIA:
MAC, topical, and peribulbar blockCOMPLICATIONS:
NonePrior to the date of surgery, the risks, benefits, and alternatives of the planned procedure were discussed with the patient, and informed consent was obtained. The patient was identified in the preoperative area by the attending physician, and the operative eye was marked. The patient was taken to the operative suite and given IV sedation and topical ocular anesthesia. A peribulbar block consisting of a 50:50 mixture of mepivacaine and bupivacaine was given. The operative eye was prepped and draped in the usual sterile ophthalmic fashion. A lid speculum was inserted.
A 23-gauge infusion cannula was inserted in the inferotemporal quadrant using the self-retaining port. Placement in the vitreous cavity was confirmed using direct visualization, then infusion was initiated. Self-retaining 23-gauge cannulas were inserted in the superonasal and superotemporal quadrants. The light pipe and vitrector were inserted into the vitreous cavity. A posterior vitreous detachment [was/was not] present. [A limited core vitrectomy was performed. Using the vitrector on gentle suction, the posterior hyaloid was carefully engaged, and posterior vitreous detachment was created.] A core vitrectomy was performed, followed by a peripheral shave vitrectomy over 360 degrees.
The peripheral retina was meticulously inspected with scleral depression, and there were no retinal breaks present. A complete air-fluid exchange was performed with **% ** gas to physiologic pressure by finger tension. The ports were removed, and the sclerostomies were inspected and found to be watertight. The eye remained physiologic pressure by finger tension. Subconjunctival antibiotic was injected into the inferior fornix. The speculum and drapes were removed, antibiotic-steroid drops were placed in the eye, and a shield was placed over the eye. The patient was then transported to the recovery unit in stable condition.