Surgeon: Reza Razeghinejad, MD | Year: 2019
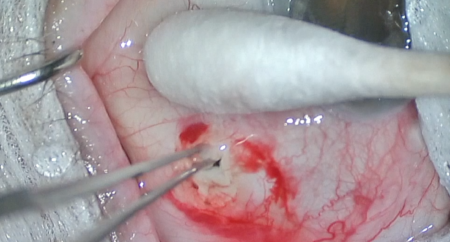
Dr. Razeghinejad performs a gonioscopy-assisted transluminal trabculotomy (GATT) for a patient with uveitic glaucoma. The trabecular meshwork is visualized with a gonioprism then incised with an MVR blade to access Schlemm’s canal. A prolene suture is threaded through the canal 360 degrees and back into the anterior chamber. Placement within the canal and absence of PAS is confirmed with gonioscopy. One end of the suture is held in the anterior chamber while the other is pulled from the eye to complete a 360-degree trabeculotomy. The viscoelastic is removed, and the chamber is pressurized to limit bleeding from the angle.
PREOPERATIVE DIAGNOSIS:
Glaucoma, *** eyePOSTOPERATIVE DIAGNOSIS:
SamePROCEDURE PERFORMED:
Gonioscopy-assisted transluminal trabeculotomy, *** eyeATTENDING SURGEON:
***ASSISTANT SURGEON:
***ANESTHESIA:
MAC, topical, and localCOMPLICATIONS:
NonePrior to the date of surgery, the risks, benefits, and alternatives of the planned procedure were discussed with the patient, and informed consent was obtained. The patient was identified in the preoperative area by the attending physician, and the operative eye was marked. The patient was taken to the operative suite and given IV sedation and topical ocular anesthesia. A retrobulbar block was given using 4 mL of equal parts 2% lidocaine and 0.75% bupivacaine. The operative eye was then prepped and draped in the usual sterile ophthalmic fashion. A lid speculum was inserted.
A Supersharp blade was used to create a paracentesis superiorly and inferiorly. Lidocaine was injected into the anterior chamber, followed by viscoelastic. A keratome was used to create a clear corneal incision. A gonioprism was used to visualize the nasal trabecular meshwork. A 23-gauge MVR blade was used to create a goniotomy. A 5-0 nylon suture was threaded through the goniotomy into Schlemm’s canal then advanced 360 degrees around the canal and back into the anterior chamber. One end of the suture was held in the anterior chamber with forceps, and the other end was pulled through a paracentesis to complete a 360-degree trabeculotomy. The I/A handpiece was then used to remove residual viscoelastic.
The corneal incisions were hydrated with balanced salt solution then inspected with a Weck-cel sponge and found to be watertight with good intraocular pressure by finger tension. The speculum and drapes were removed, and antibiotic-steroid drops were placed in the eye. A patch and shield were applied. The patient was then transported to the postoperative care unit in good condition.