Surgeon: Reza Razeghinejad, MD | Narrator: Lindsay Machen, MD | Year: 2019
Dr. Razeghinejad performs a cataract extraction and Baerveldt valveless glaucoma drainage device implantation. A stenting suture and ligature suture are placed, then the tube shunt plate is secured in place. A pericardial patch graft is positioned to protect the tube, then the conjunctiva is closed with Vicryl sutures.
PREOPERATIVE DIAGNOSES:
1. Cataract, *** eyePOSTOPERATIVE DIAGNOSES:
SamePROCEDURES PERFORMED:
1. Phacoemulsification cataract extraction with intraocular lens implantation, *** eyeATTENDING SURGEON:
***ASSISTANT SURGEON:
***IMPLANTS:
1. *** *** diopters, serial number ***, aim ***ANESTHESIA:
MAC, topical, and localCOMPLICATIONS:
NonePrior to the date of surgery, the risks, benefits, and alternatives of the planned procedure had been discussed with the patient, and informed consent had been obtained. The patient was identified in the preoperative area by the attending physician, and the operative eye was marked. The patient was transported to the operative suite and given IV sedation and topical ocular anesthesia. The operative eye was prepped and draped in the usual sterile ophthalmic fashion. A lid speculum was inserted to provide adequate exposure.
A paracentesis was made into clear cornea. Epi-Shugarcaine and viscoelastic were injected into the anterior chamber. A clear corneal incision was made using a keratome. A cystotome was used to initiate a capsular flap, and Utrata forceps were used to create a continuous curvilinear capsulorrhexis. Hydrodissection was performed using balanced salt solution on a blunt tipped cannula. A phacoemulsification handpiece was used to disassemble and remove the lens nucleus. An irrigation/aspiration handpiece was used to remove the remaining cortical material and polish the capsule. The anterior chamber and capsular bag were filled with viscoelastic. The intraocular lens was placed into the bag and dialed into position.
Attention was then directed to the superior cornea and conjunctiva. A 7-0 Vicryl traction suture was placed in partial thickness superior cornea, and the eye was rotated infranasally. A superior limbal conjunctival opening was made using Wescott scissors. Bupivacaine was injected into the subconjunctival space and spread using a blunt instrument. A peritomy was made temporally through superiorly with radial relaxing incisions. Blunt dissection was performed with Westcott scissors to expand the pocket underlying conjunctiva and Tenon’s. A peribulbar block was given using bupivacaine. Gentle cautery was performed to achieve hemostasis at the intended site of tube entry.
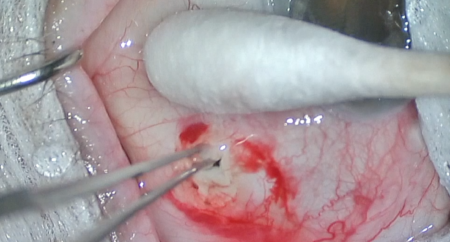
The superior and lateral rectus muscles were isolated using a muscle hook. The Baerveldt implant was prepared with a Latina suture and a 7-0 Vicryl suture closure. The tube was primed with balanced salt solution and showed stable occlusion by the 7-0 Vicryl suture. The implant was secured under the superior and lateral rectus muscles approximately 8-10 mm posterior to the limbus. The tube was then secured with two 10-0 nylon sutures and trimmed in beveled fashion. A 23-gauge bent needle was used to create a tunneled sclerostomy that entered the anterior chamber above the iris plane but deep to the corneal endothelium. The tube was inserted through this tract, positioned appropriately in the anterior chamber, then secured to the sclera with a 10-0 nylon suture. The Tutoplast processed pericardial patch graft was secured over the exposed tube with 7-0 Vicryl suture. The conjunctiva was advanced using smooth forceps and secured at the limbus with 7-0 Vicryl interrupted and running sutures.
The traction suture was removed. The corneal incisions were hydrated with balanced salt solution then inspected with a Weck-cel sponge and found to be watertight with good intraocular pressure by finger tension. The tube was inspected and found to be in good position with respect to the cornea, iris, and lens. The speculum and drapes were removed, and antibiotic-steroid drops were placed in the eye. A patch and shield were applied. The patient was then transported to the postoperative care unit in good condition.