Surgeon: Jonathan Myers, MD | Year: 2020
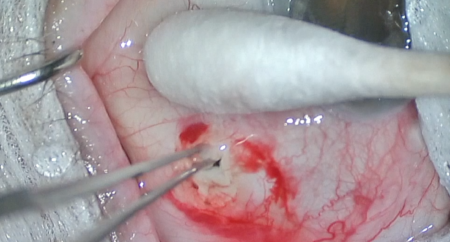
Dr. Myers demonstrates ab externo implantation of a Xen Gel Stent. The conjunctiva is marked 3 mm posterior to the limbus. The injector enters the subconjunctival space 5 mm posterior to the limbus, advanced to the 3 mm mark, then directed inferiorly through the sclera into the anterior chamber. The location of the injector is confirmed with a gonioprism. The Xen Gel Stent is deployed into position with concurrent retraction of the injector. Mitomycin-C is then injected subconjunctivally around the stent.
PREOPERATIVE DIAGNOSIS:
Glaucoma, *** eyePOSTOPERATIVE DIAGNOSIS:
SamePROCEDURE PERFORMED:
Xel Gel Stent implantation with mitomycin-C, *** eyeATTENDING SURGEON:
***ASSISTANT SURGEON:
***IMPLANT:
Xel Gel Stent, serial number ***ANESTHESIA:
MAC, topical, and localCOMPLICATIONS:
NonePrior to the date of surgery, the risks, benefits, and alternatives of the planned procedure were discussed with the patient, and informed consent was obtained. The patient was identified in the preoperative area by the attending physician, and the operative eye was marked. The patient was taken to the operative suite and given IV sedation and topical ocular anesthesia. The operative eye was prepped and draped in the usual sterile ophthalmic fashion. A lid speculum was inserted.
A 7-0 Vicryl traction suture was placed in partial-thickness superior cornea, and the eye was rotated inferiorly. A 1:1 mixture of preservative-free 1% lidocaine and mitomycin-C (0.4 mg/mL) was injected into the subconjunctival space. A superotemporal paracentesis was made into clear cornea. The Xen Gel Stent was marked with a marking pen. The injector was introduced into the superior subconjunctival space distal to the intended scleral entry site, advanced to 3 mm posterior to the limbus, then directed inferiorly through sclera into the anterior chamber angle. The stent was then deployed into the anterior chamber and subconjunctival space with concurrent retraction of the injector. A direct gonioprism was used to confirm the correct position in the angle. An appropriate bleb was noted to form over the subconjunctival portion of the stent.
The traction suture was removed. The corneal incision was hydrated then inspected with a Weck-cel sponge and found to be watertight with good intraocular pressure by finger tension. The speculum and drapes were removed, and antibiotic-steroid drops were placed in the eye. A shield was applied. The patient was then transported to the postoperative care unit in good condition.