Surgeon: Christopher Rapuano, MD | Year: 2019
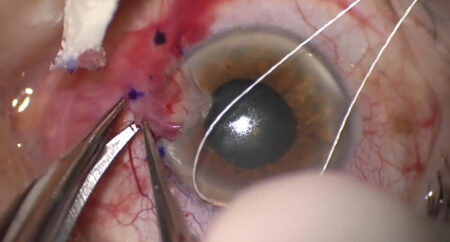
Dr. Rapuano performs a Descemet stripping endothelial keratoplasty (DSEK) for a patient with Fuchs’ dystrophy.
PREOPERATIVE DIAGNOSIS:
Corneal edema, *** eyePOSTOPERATIVE DIAGNOSIS:
SamePROCEDURE PERFORMED:
Descemet stripping endothelial keratoplasty, *** eyeATTENDING SURGEON:
***ASSISTANT SURGEON:
***SPECIMEN:
Corneal tissue, sent to PathologyIMPLANT:
Corneal tissue from ** eye bank, serial number ***ANESTHESIA:
MAC and topicalCOMPLICATIONS:
NonePrior to the date of surgery, the risks, benefits, and alternatives of the planned procedure were discussed with the patient, and informed consent was obtained. The patient was identified in the preoperative area by the attending physician, and the operative eye was marked. The patient was taken to the operative suite and given IV sedation and topical ocular anesthesia. The operative eye was prepped and draped in the usual sterile ophthalmic fashion. A lid speculum was inserted.
The eye was measured, and the decision was made to use a *** mm trephine for the donor cornea. A conjunctival window was made inferonasally, then a mixture of 2% lidocaine with 0.5% Marcaine was injected into the sub-Tenon space. A SuperSharp blade was used to make four corneal paracenteses. Lidocaine then viscoelastic were injected into the anterior chamber. A guarded diamond blade set to a depth of 300 microns was used to make a 4 mm groove at the temporal limbus. A crescent blade was used to extend this wound into clear cornea. A 2.4 mm keratome was then used to extend the wound into the anterior chamber.
The corneal trephine was used to inscribe a circle onto the corneal epithelium. Next, a reverse Sinskey hook was used to score Descemet membrane. A Descemet stripper was used to remove Descemet membrane without complications. All viscoelastic was removed from the anterior chamber using the irrigation/aspiration handpiece. An anterior chamber maintainer was placed in a nasal paracentesis. The wound was enlarged to approximately 4 mm, then four para-axial corneal vent incisions were then created using a SuperSharp blade.
Attention was then directed to the donor cornea. The button was punched to the diameter noted above, loaded onto the Busin glide, then carefully implanted into the anterior chamber and centered. The wound was closed with three 10-0 nylon sutures, and the knots were buried. The anterior chamber maintainer was then removed. An air bubble was injected under the graft. The venting incisions were burped, and a high-pressure fill was performed for 10 minutes. Finally, a partial air-fluid exchange was performed so that the bubble was just covering the entire diameter of the graft.
At the end of the case, the anterior chamber had an 80% air fill, all wounds were watertight, and the graft was in excellent position. The speculum and drapes were removed, cycloplegic and antibiotic-steroid drops were placed in the eye, and a shield was placed over the eye. The patient was then transported to the recovery unit in stable condition. They stayed supine for one hour then were examined at the slit lamp. The graft was well centered, the air bubble was above the inferior margin of the pupil, and the eye was at physiologic pressure.