Surgeon: Beeran Meghpara, MD | Year: 2019
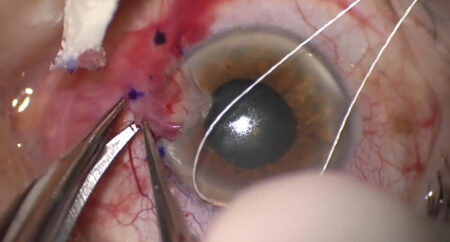
Dr. Meghpara performs a deep anterior lamellar keratoplasty (DALK) in a patient with keratoconus.
PREOPERATIVE DIAGNOSIS:
***, *** eyePOSTOPERATIVE DIAGNOSIS:
SamePROCEDURE PERFORMED:
Deep anterior lamellar keratoplasty, *** eyeATTENDING SURGEON:
***ASSISTANT SURGEON:
***SPECIMEN:
Corneal tissue, sent to PathologyIMPLANT:
Corneal tissue from ** eye bank, serial number ***ANESTHESIA:
MAC and topicalCOMPLICATIONS:
NonePrior to the date of surgery, the risks, benefits, and alternatives of the planned procedure were discussed with the patient, and informed consent was obtained. The patient was identified in the preoperative area by the attending physician, and the operative eye was marked. The patient was transported to the operative suite and given IV sedation and topical ocular anesthesia. The operative eye was prepped and draped in the usual sterile ophthalmic fashion. A lid speculum was inserted to provide adequate exposure.
The cornea was measured with calipers, then the decision was made to use a *** mm Hessburg-Barron corneal vacuum trephine and a *** mm donor graft punch. An RK marker was used to mark the cornea. The corneal vacuum trephine was used to trephine the cornea to 90% thickness. A paracenteses was created at the temporal limbus, and a 10% air bubble was injected into the anterior chamber. A 27-gauge needle was used to initiate a stromal tunnel, and a Sarnicola dissector was used to complete a deep stromal tunnel to the central cornea. A Sarnicola cannula was then inserted into the tunnel, and air was injected rapidly to create a “Big Bubble”. Bubble formation was confirmed by peripheralization of the anterior chamber bubble.
The anterior 70% of the cornea was removed using a crescent blade. The stroma was marked centrally, and viscoelastic was applied over the mark. A SuperSharp blade was then used to create an incision into the air-filled space. Viscoelastic was injected into the pre-Descemet space. The remaining stroma was removed using curved corneal scissors.
Attention was directed to the donor graft tissue. The endothelium was stained with trypan blue and removed using a stripping technique. The cornea was then punched to the diameter described above. The graft was then brought into the operating field and sutured into position using 16 interrupted 10-0 nylon sutures. All sutures were rotated and buried.
The wounds were checked and found to be watertight, and eye was physiologic pressure by finger tension. Subconjunctival steroid and antibiotic injections were placed into the inferior fornix. The speculum and drapes were removed, antibiotic-steroid drops were placed in the eye, and a shield was placed over the eye. The patient was then transported to the recovery unit in stable condition.